Diabetic Retinopathy: Causes, Stages, and the Latest Treatments for Vision Preservation
Diabetic Retinopathy: Causes, Stages, and the Latest Treatments for Vision Preservation
"Amid the vastness of life's challenges, serenity within is our strongest shield."
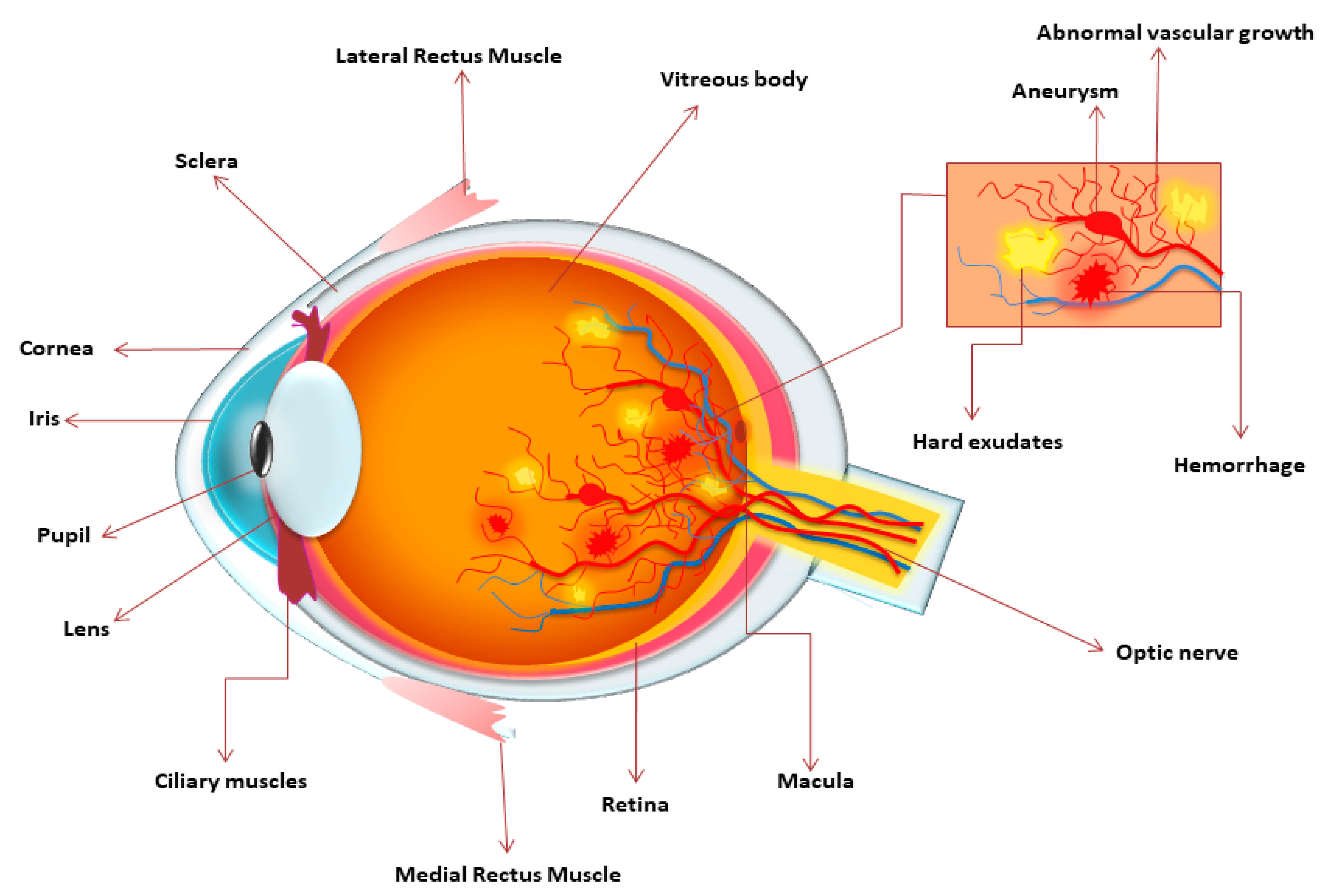
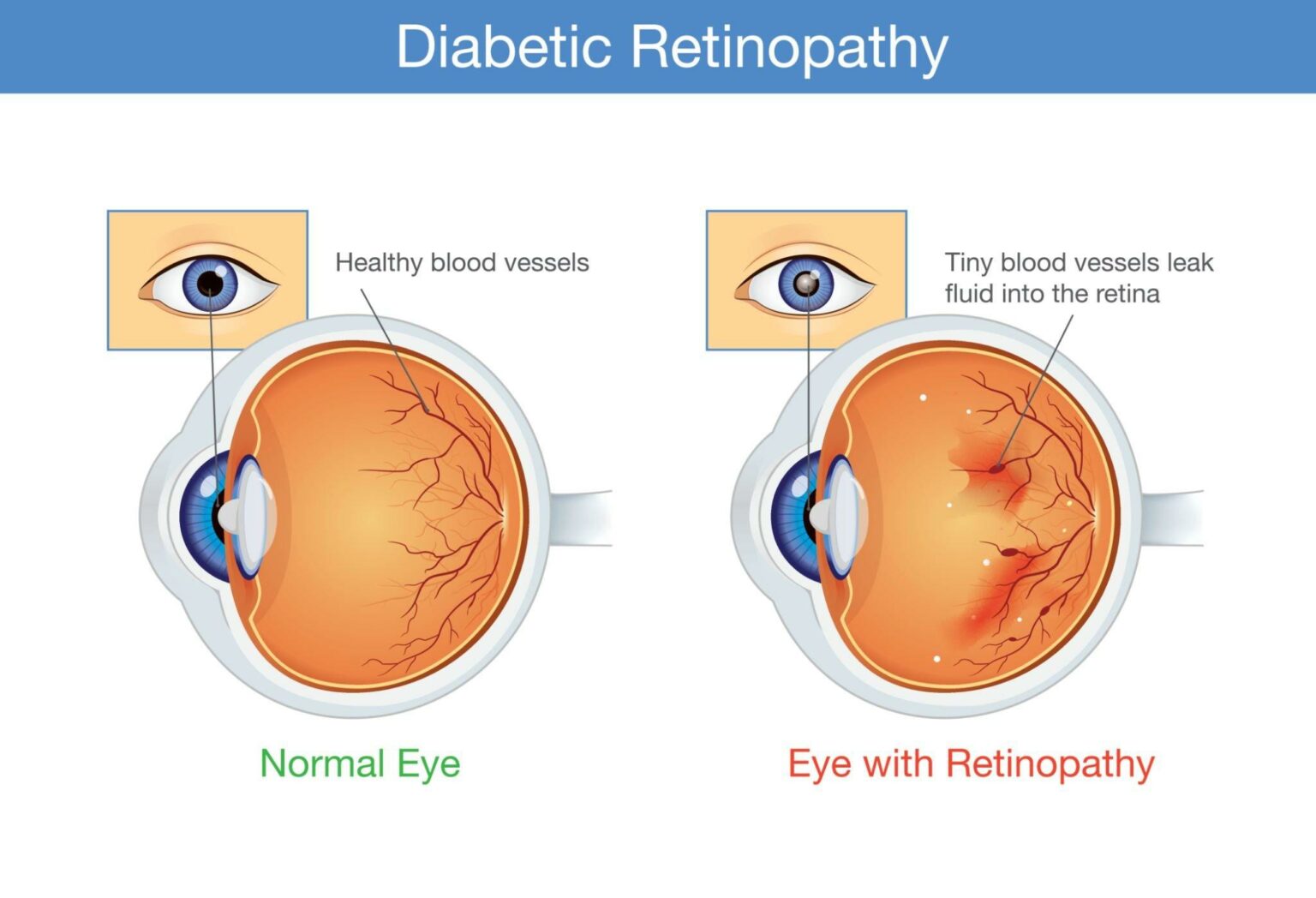
Diabetic Retinopathy (DR) is a common microvascular complication of diabetes and one of the leading causes of blindness in working-age adults globally. It is characterized by progressive damage to the small blood vessels of the retina due to chronic hyperglycemia. DR is often accompanied by neuroglial dysfunction and can result in irreversible vision loss if untreated.
DR is primarily caused by prolonged high blood sugar levels which damage retinal capillaries. Key risk factors include:
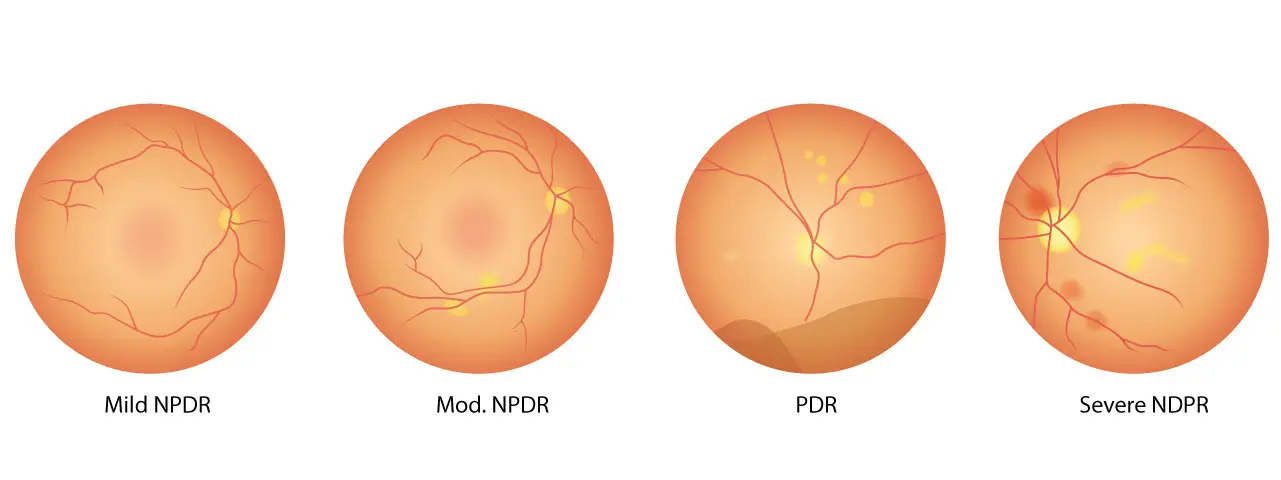
DR is categorized into:
NPDR Stages:
PDR Stages:
DME Types:
According to the International Diabetes Federation (IDF), over 537 million adults (20–79 years) had diabetes in 2021, projected to rise to 783 million by 2045. An estimated 103 million adults globally had DR in 2020, expected to reach 160 million by 2045.
In China, DR prevalence among diabetics is around 22.4%, with higher rates in northern and rural areas. The highest prevalence is among individuals aged 50–59 years.
A comprehensive ophthalmic evaluation includes medical history, visual acuity, intraocular pressure measurement, dilated fundus examination, and optical coherence tomography (OCT). Fundus photography (ETDRS 7-field or ultra-wide field imaging) helps in DR staging.
For systemic evaluation, it is essential to review diabetes duration, glycemic control, and comorbidities like hypertension and dyslipidemia.
Treatment includes both systemic management (glycemic, blood pressure, and lipid control) and ocular-specific interventions depending on DR stage and presence of DME.
Panretinal photocoagulation is a cornerstone for high-risk PDR and severe NPDR. It reduces the risk of severe vision loss. When DME coexists, anti-VEGF is often administered before PRP.
Intravitreal anti-VEGF agents are first-line treatments for DME and effective in reducing neovascularization in PDR. Common drugs include:
These drugs effectively reduce vascular leakage, promote visual improvement, and delay disease progression.
Used when anti-VEGF response is inadequate. Options include:
Steroids modulate inflammation and help restore the blood-retinal barrier.
Indicated in:
Combining PPV with anti-VEGF enhances outcomes. Not first-line for DME unless traction or severe non-resolving edema persists.
Diabetic patients are more prone to early-onset cataracts. Pre-operative DR stabilization is essential. If DME is present, treat with anti-VEGF or corticosteroids concurrently with cataract surgery.
As of July 2025, over 452 drugs are under development for DR. Key players include:
These developments promise safer and more effective treatments for DR in the future.

Diabetic Retinopathy is a major threat to vision but is manageable with early diagnosis, comprehensive treatment, and regular follow-up. Integrated systemic and ocular therapies, along with advancements in pharmacology, offer hope for preserving sight in diabetic individuals.
Let awareness lead to action—because every blink is worth protecting.
Categories: health